
Treatment
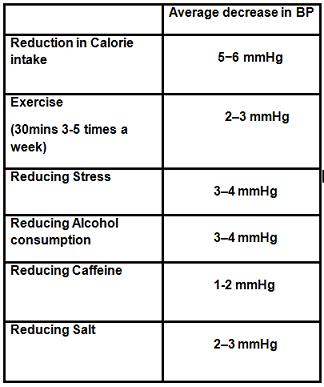
There are a range of treatments availiable for hypertension. In milder cases there are many lifestyle changes which can be made in order to reduce blood pressure and bring it closer to the ideal range as demonstrated by the table below.
Choice of medication is dependent on a number of factors including age,race and pre-existing medical conditions. Patients with blood pressure above160/100 mmHg or those that have an elevated risk of cardiovascular disease are prescribed drugs.
In patients under the age of 55 ACE inhibitors are the first choice in managing the condition. Patients that are over 55 and/or Afro-Caribbean thiazide diuretics and calcium channel blockers are the drugs of choice as ACE inhibitors are less effective in this group of people.
ACE inhibitors
Renin produced by the kidney when blood volume is low increases blood pressure this results in the production of Angiotensin I which is converted into the vasoconstrictor Angiotensin II by Angiotensin converting enzyme (ACE).See Renin -Angiotensin pathway. Angiotensin II is responsible for stimulating thirst and the production of aldosterone which promotes retention of salt and water. This fluid retention also increases blood pressure.
The mechanism of action is to block the Angiotensin II converting enzyme which prevents the production of Angiotensin II. The arteries are no longer constricted and there is increased blood flow.
Examples include Ramipril, Enalapril and Perindopril
Thiazide Diuretics
Mode of action is to block sodium reabsorption at the distal convoluted tubule.Bendroflumethiazide and indapamide are often referred to as ‘water tablets’ and work by increasing urine production by binding to the Cl- site of the Na+/Cl-co- transporter so sodium is not reabsorbed and instead is excreted.
Examples include Bendroflumethiazide, Indapamide and Clopamide
Angiotensin-II receptor antagonists
These drugs prevent the production of Angiotensin II which causes vasoconstriction. By blocking the production of angtiotensin II the production of aldosterone is also reduced. Unlike the ACE inhibitor these do not have a side effect of a dry cough.
Examples include Valsartan, Candesartan and Losartan
Calcium Channel Blockers
Dihydropyridines, phenylalylamines and benzothiazepines are classes of antagonists of the L-type calcium channel. Involved in the plateau phase of the cardiac action potential they reduce influx of calcium entering the cell. They have a vasodilatory effect on the blood vessels as peripheral resistance is reduced. Consequently contractility of the heart is decreased and so is myocardial oxygen demand. Cardiac output largely remains unaffected.
Examples include Amlodipine, Nifidepine and Diltiazem
Selective α1 antagonists
These drugs block the α1adrenoceptors and cause vasodilatation and a decrease in arterial pressure. Unfortunately studies have shown these drugs to e ineffective at prevent stroke or MI. Side effects include impotence and hypotension.
Examples include Doxazosin, Prazosin and Terazosin
Beta Blockers
Beta blockers are no longer routinely used for hypertension as there are more effective drugs now on the market. They are used mainly in treating heart failure. Studies have also shown that beta blockers are 30% more likely to induce type 2 diabetes than other antihypertensive. Their mode of action is to decrease sympathetic stimulation of heart. In the kidney beta blockers decrease secretion of renin and therefore reduce angiotensin II (vasoconstriction)
Examples included Atenolol, Propranolol and Timolol
Search site
Did You Know?
One third of patients with hypertension are overweight. 75% of patients with diabetes develop cardiovascular dieases due to hypertension. There are also strong links between insulin resistance and hypertension.